Abstract:
Bangladesh’s health care system, particularly in rural areas, experiences enormous obstacles in
providing complete preventive and primary healthcare services due to the lack of adequate healthcare facilities,
resource constraints, and a non-functional referral system. To alleviate these problems, in this study, we introduce
the digital general practitioner (GP) model for rural Bangladesh, digital platforms and present a statistical
analysis of the data that was gathered from the pilot project.
Methods: A total of 12,746 people were provided regular health services during the pilot project, from all genders
and age groups, and provided their socio-demographic and healthcare-related data. We analyzed healthcarerelated
data by carrying out both descriptive and inferential statistics.
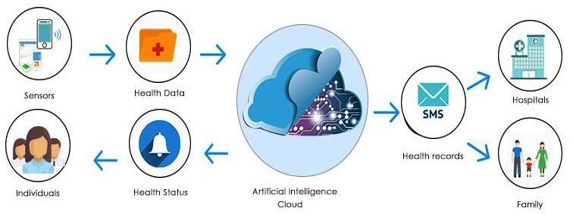
Results: By utilizing this digital GP model, rural residents can receive routine health screenings at their homes,
identify health risks early, receive consultation and health education, and be referred to GP and upper-level
health facilities as needed. We found that hypertension was more prevalent (4.84% of the served population),
and cancer was the least prevalent of all the NCDs in the studied population (0.05% of the served population).
The population for stroke, hypertension, diabetes increased until the 50–59 age range as age increased, following
which the population proportion declined as age increased. Additionally, 3.96% of young females were severely
malnourished, comparably higher proportion than young males (2.34%).
Conclusion: NCDs such as hypertension, diabetes was prevalent among rural people. Necessary steps should be
taken to raise preventive and primary healthcare awareness among rural people.
Public interest summary: The absence of proper healthcare facilities, resource constraints, and a non-functional
referral system hamper Bangladesh’s health care system’s ability to provide comprehensive preventive and
primary healthcare services in rural area. As a result, patients develop advanced ailments, including noncommunicable
diseases (NCDs), and must seek treatment at an expensive specialty hospital. To resolve this
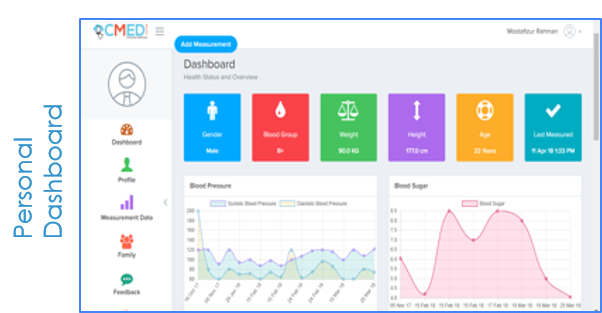
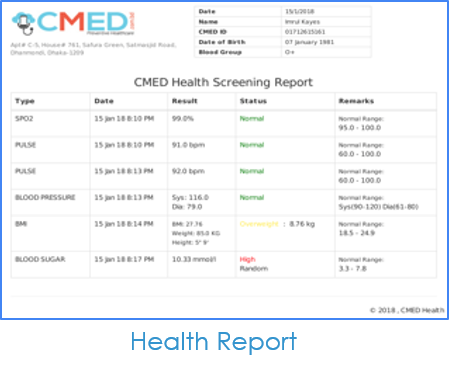
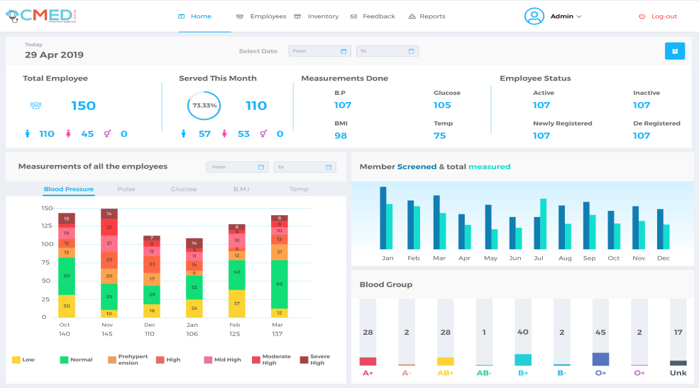
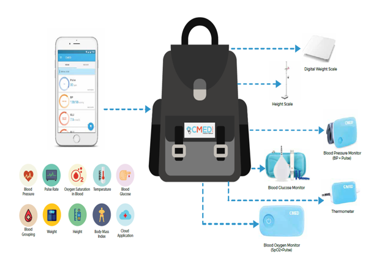
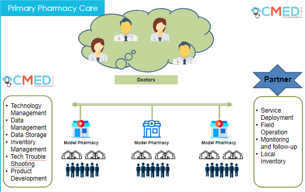
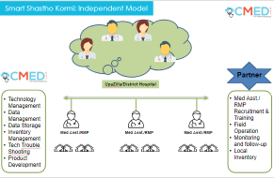
issue, we introduce a digital GP model for rural Bangladesh, then show digital platforms that use the concept, and
lastly summarize significant findings from the piloted digital GP model. By utilizing this digital GP model, rural
residents can receive routine health screenings at their homes, identify health risks early, receive consultation
and health education, and be referred to GP and upper-level health facilities as need. From our data analysis, we
discovered high burden of NCDs such as hypertension and diabetes in the piloted area. Necessary steps should be
taken to raise preventive and primary healthcare awareness among rural people.